Male and female facial ageing patterns can differ, but they are not treatment rules. Bone structure, skin thickness, fat distribution, facial hair, expression and hormones can influence how change appears. Corey Anderson RN assesses the individual face, medical history, previous treatment, expectations, risk and consent before discussing whether planning, waiting, referral or no treatment is more appropriate.
Planning Goals And Individual Variation
Natural looking planning goals should be described as aims, not promises. Corey considers individual variation, facial balance, proportion and restraint before deciding whether a plan is clinically appropriate.
This keeps the discussion grounded in anatomy, timing, consent, risk and realistic expectations rather than a promised cosmetic outcome.
Patterns Are Not Rules
Some people have stronger brow or jaw structure. Some have thinner skin, greater sun damage, more expressive movement or different lower face support. These differences do not map neatly onto every man or every woman.
A consultation should never assume that a person needs a certain plan because of gender. It should assess anatomy and suitability directly.
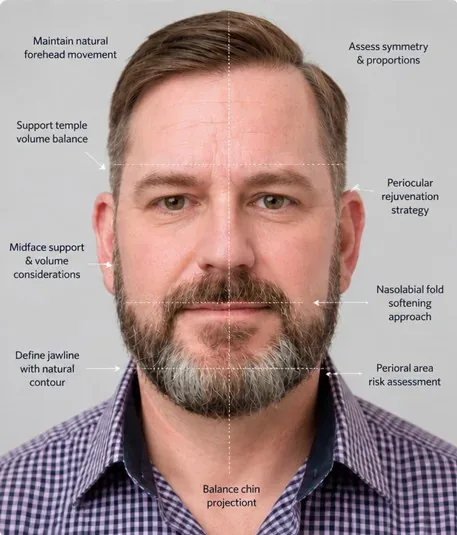
Facial Structure And Proportion
Facial ageing is influenced by bone structure, soft tissue support, skin quality and movement. The brow, cheek, chin, jawline and lip area can change how tiredness, heaviness, hollowing or imbalance is perceived.
For some patients, the concern they notice in one area is partly caused by support or proportion in another area.
Skin Quality And Ageing Timing
Skin quality varies widely. Sun exposure, genetics, smoking history, weight change, hormones, medical history and skin care can all affect texture, elasticity and visible lines.
Because these factors vary, the useful question is not whether a male or female pattern is present. It is what is contributing to this patient’s concern.
Expression And Brow Position
Expression patterns can affect forehead lines, frown lines, crow’s feet, brow heaviness and the way tiredness is read on the face. Brow position and eyelid history also matter.
Corey assesses facial movement at rest and during expression before discussing whether treatment is suitable.
Lower Face, Chin And Jawline
The lower face can influence how ageing appears around the mouth, jawline and chin. Jawline strength, chin support, dental context, skin quality and lip proportion may all contribute to what the patient notices.
This is why facial ageing assessment should consider relationships across the face rather than one isolated feature.
Why Individual Assessment Matters More
Clinical categories can help explain patterns, but they should not decide treatment. A person may not fit the expected pattern, may have a medical reason to avoid treatment or may simply want information rather than a procedure.
The consultation reviews the concern, history, anatomy, expectations, risk and whether any intervention is appropriate.
Treatment Planning Is Not A Formula
Aesthetic planning should not be based on male or female templates. It should consider the concern, facial structure, movement, skin quality, previous treatment, timing, consent and the patient’s comfort with change.
The outcome may be treatment planning, waiting, referral, skin focused advice or no treatment.
When Waiting Or No Treatment Makes Sense
Waiting or no treatment may be recommended if risk is higher, timing is poor, expectations are not realistic, previous treatment needs review, symptoms need medical assessment or the concern is better managed another way.
A recommendation not to treat is part of responsible care.
What Patterns Can Differ Between Faces?
Broad patterns can differ, but Corey does not use sex or gender as a treatment formula.
- Bone structure, brow shape, jawline width, chin support and facial proportions can affect visible ageing.
- Skin thickness, sun exposure, shaving, facial hair, pigment and texture can change how concerns appear.
- Fat distribution, weight change, facial movement and previous treatment can alter support and shadows.
- Personal goals, medical history and risk matter more than category based assumptions.
How Should Inclusive Assessment Work?
Assessment should be individual, respectful and clinically grounded. The consultation should not force a person into a fixed aesthetic category.
- Corey asks what the patient notices and what they want to understand.
- The face is assessed at rest and with movement, with attention to proportion and natural variation.
- Suitability, consent, risks, limits and aftercare are discussed before any treatment decision.
- Waiting, referral, staged review or no treatment remain valid outcomes of consultation.
What Should You Verify Before Booking?
Before using this page to choose a next step, check that the clinic and practitioner details are clear and accountable.
- Core Aesthetics consults from 12A Atherton Road, Oakleigh.
- Consultations are led by Corey Anderson RN, Registered Nurse.
- Corey can be checked on the Ahpra public register using registration number NMW0001047575.
- This page was reviewed on 8 June 2026 for consultation-first wording, suitability language, risk framing and consent language.
- The same practitioner model means assessment, planning and review are connected rather than separated across multiple providers.
Use the verification page if you want to confirm practitioner and clinic details before booking.
When Should You Book Or Wait?
Book a consultation when you want an individual assessment rather than a self selected treatment. Same-day treatment is not automatic. It should only be discussed when assessment, suitability, risk discussion, informed consent and clinical judgement support proceeding.
Waiting, planned review, referral or no treatment may be the responsible recommendation. If the concern is sudden, painful, one-sided, medically unusual or changing quickly, seek appropriate medical advice before cosmetic planning.
For next steps, use book a consultation, contact the clinic, treatment suitability assessment and why no treatment may be recommended.
Useful Next Pages
For men considering consultation, read men’s aesthetics Melbourne, male aesthetic consultation and the men’s aesthetic options guide. For lower face context, see jawline treatment Melbourne and chin treatment Melbourne.
For decision support, read treatment suitability assessment.

Book A Consultation
If you want to understand your own facial ageing pattern, book a consultation with Corey at Core Aesthetics in Oakleigh. The appointment can clarify what is contributing to the concern and whether any next step is appropriate.
Is this for you?
Consider booking a consultation if
- You are an adult wanting to understand facial ageing assessment
- You want broad ageing patterns explained without assumptions about your face
- You value informed consent, risk discussion and realistic expectations
- You are open to waiting, referral, staged review or no treatment where appropriate
This may not be for you if
- You want a promised appearance change before assessment
- You want treatment without informed consent, risk discussion or aftercare planning
- You have active skin inflammation, eye symptoms, unhealed skin or unresolved medical concern in the area to be assessed
- You are seeking treatment because of pressure from another person or an urgent event
Suitability is confirmed at consultation. This list is general guidance, not a substitute for clinical assessment.
Frequently asked questions
Do male and female facial ageing patterns differ?
They can. Facial structure, skin quality, expression patterns, hormones, sun exposure, genetics and lifestyle can all influence how ageing appears. Individual assessment matters more than any category.
Does this mean men need a different treatment plan?
Not automatically. A plan should be based on the person’s anatomy, concern, medical history, expectations, risk, consent and suitability rather than a gender label. Broad patterns can inform assessment, but they should not determine treatment.
What matters more than male or female categories?
Corey assesses facial structure, movement, resting lines, skin quality, previous treatment, medical history, timing, expectations and risk factors. The aim is to understand the individual face before discussing treatment planning, waiting, referral or no treatment.
Can women read this page too?
Yes. The page uses male and female comparisons for clinical literacy, but Core Aesthetics assesses every patient individually and respectfully. The same consultation-first approach applies across anatomy, goals, identity, suitability and consent.
Why does brow position matter?
Brow position can affect how upper face lines, heaviness and tiredness are assessed. It can also change how expression and resting appearance are interpreted, so it needs individual review before any treatment decision is discussed.
Why does the lower face matter?
Jawline, chin, dental support, cheek support and skin quality can all affect how ageing appears. Focusing on one feature alone may miss the real contributor.
Can treatment happen on the same day?
Some adult patients may be suitable for same day treatment, but only after assessment, informed consent, risk discussion and clinical judgement support proceeding. Consultation may also lead to waiting, referral, review or no treatment.
Can Corey recommend no treatment?
Yes. Corey may recommend waiting, referral, review of another concern or no treatment if that is more appropriate after assessment. No treatment can be the responsible recommendation when benefit is unclear or risk is not justified.
What makes men’s aesthetic consultation different from choosing a treatment from a list?
Corey assesses the concern in the context of the whole face, not as an isolated search phrase. The consultation covers anatomy, goals, safety, alternatives, consent and whether doing less or waiting would be more appropriate.
Why are photos not enough to decide whether men’s aesthetic consultation is suitable?
For men’s aesthetic consultations, Corey considers facial structure, expression, skin quality and the patient’s own goal rather than assuming a masculine or trend based result. Photos can help someone explain a preference, but they cannot confirm suitability. Lighting, anatomy, expression, previous treatment and editing can mislead, so assessment matters more than comparison images.